|
Near and Intermediate Visual Acuityin Clinical Studies with Multifocal Intraocular Lenses |
|
|
|
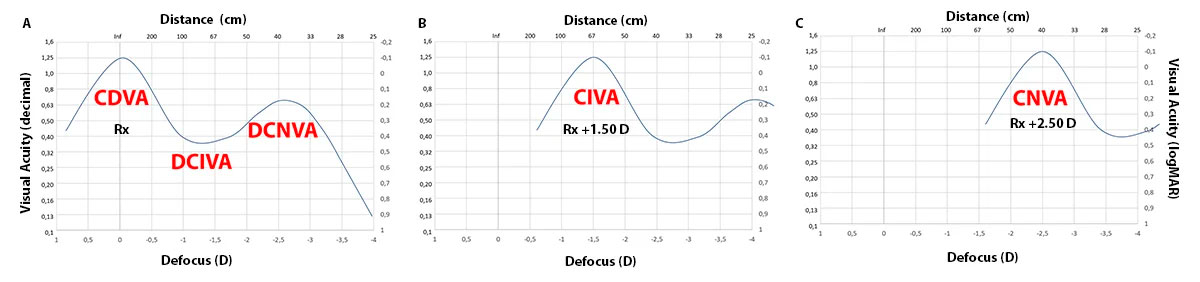
DCIVA and DCNVA are the standardized abbreviations for the measurement of visual acuity at intermediate and near distances when the patient is corrected with best spectacle correction for an infinite distance.[1] CIVA and CNVA are the abbreviations for visual acuity at intermediate and near when the patient is corrected with best spectacle correction for each of these distances.[1] Protocols for clinical studies should be designed to include the minimum number of tests that maximize the information obtained. Failure to understand the purpose of why certain visual performance measures are taken can lead to the development of clinical trial protocols with long duration and therefore unreliable data due to patient fatigue. Many clinical studies include visual acuity with the best near and intermediate correction (CNVA and CIVA) with multifocal intraocular lenses, even these variables are included in the international standards of Clinical Studies[2]. In our opinion, these measures are a clear example of redundant measures that increase evaluation times providing little or no additional information. Why is the information redundant?PTo explain why we're going to base it on the defocus curve. In the image you can see the relationship between the positions of the defocus curve and each of these abbreviations. Figure A shows how the patient with best infinity correction will have the peak of maximum vision at 0 D on the defocus curve. The abbreviations DCIVA and DCNVA correspond to the -1.50 D (67 cm) and -2.50 D (40 cm) curve positions.
When we seek to measure the CIVA and CNVA what we do is to place the addition that optimizes the vision of the patient at intermediate and near distances, considering that the peak of best vision is at 0 D, placing an addition of +1.50 D would optimize the vision at 67 cm (Figure B) and with +2.50 D at 40 cm (Figure C), but the visual performance is the same as that obtained in the CDVA since we are measuring the visual performance provided by the same focus in different positions in a redundant way after shifting the defocus curve. Why do CDVA, CIVA and CNVA differ in clinical studies?Although in theory CDVA, CIVA and CNVA should be the same in clinical studies, the means may differ for several reasons, including:
References:
|